![]()
| Prompt | Response | Req | Len |
|---|---|---|---|
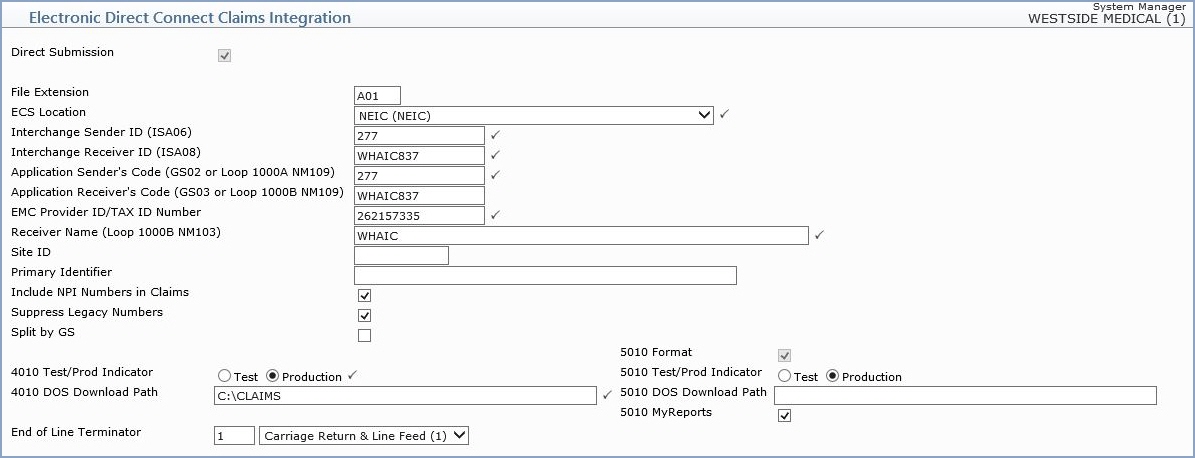
| File Extension | Type the File Extension, which is generally a letter followed by the database number. | 3 | |
| ECS Location | Select the location code that this type of claim is sent to from the Location Code list. |  |
4 |
| 4010 Test/Prod Indicator | Select the appropriate option to indicate whether the submission of claims is in the Test phase or is in Production. | |
4 |
| 4010 DOS Download Path | Type the DOS path that the claims files will be downloaded to. | |
50 |
| Interchange Sender ID | Type the Interchange Sender ID number. | |
15 |
| Interchange Receiver ID | Type the Interchange Receiver ID Number. | |
15 |
| Application Sender's Code | Type the Application Sender's code. | |
15 |
| Application Receiver's Code | Type the Application Receiver's code. | 15 | |
| EMC Provider ID/TAX ID Number | Type the unique number assigned to the provider for Electronic Medical Claims (EMC) identification purposes. | |
15 |
| Receiver Name | Type the name of the entity (insurance carrier/administrator) who will receive these claims files. | |
60 |
| Site ID | Type the Site ID. | 10 | |
| Direct Submission | If you are sending these claims directly to the payer rather than via the EMEDIX, select this check box. | |
1 |
| Primary Identifier | If filled in, this will be sent in Loop 1000B, Segment NM109 of the 5010 electronic claim file which is populated by the Receiver Code. | 80 | |
| 5010 Format | If claims are to be sent in 5010 format, select this check box. | 1 | |
| 5010 Test/Prod Indicator | Select the appropriate option to indicate whether the submission of claims is in the Test phase or is in Production. | 1 | |
| 5010 DOS Download Path | Type the DOS path that the claims files will be downloaded to. | 50 | |
| MyReports | Type the Interchange Sender ID number. | 1 | |
| Include NPI Numbers in Claims | If you want the NPI numbers from your tables to be included in the electronic claims, select this check box. | 1 | |
| Suppress Legacy Numbers | If you want to suppress all legacy numbers from being included in the electronic claims, select this check box. | 1 | |
| Hold Claims | If you want to hold claims from being submitted, select this check box. All claims for this Insurance Form Number will be held until you clear this check box. The held claims will appear on the Exception Report until they are transmitted electronically or moved to paper. | 1 | |
| Split by GS | Enter 'Y' to generate separate file per submitter (for direct sends only) | 1 |
Copyright and Trademark Notice. Copyright © 2019 CompuGroup Medical, Inc. CGM®, CompuGroup Medical® and the CGM logo are registered trademarks and CGM webPRACTICE™ and CGM webTOOLS™ are trademarks of CompuGroup Medical AG in the United States and/or other countries. Any rights not expressly granted herein are reserved.
