![]()
| Prompt | Response | Req | Len |
|---|---|---|---|
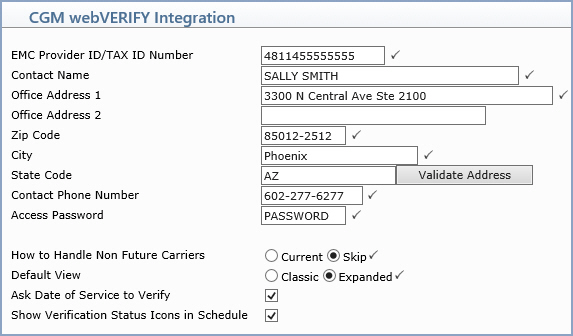
| Enabled | Check box if CGM webVERIFY is enabled. | 1 | |
| Interchange Sender ID | Type the ID number assigned to your practice. |  |
15 |
| EMC Provider ID/TAX ID Number | Type the EMC Provider ID/Tax ID Number. | |
15 |
| Contact Name | Type the contact person for CGM webVERIFY in your practice for insurance carriers to contact if needed. | |
35 |
| Office Address 1 | Type the street address for the practice. | |
40 |
| Office Address 2 | Type the zip code for the practice. | 30 | |
| Zip Code | Type the zip code for the practice. | |
9 |
| City | Type the city. | |
20 |
| State | Type the phone number for the CGM webVERIFY contact person in your practice. | 40 | |
| Contact Phone Number | Type the phone number for the CGM webVERIFY contact person in your practice. | |
12 |
| Access Password | Type the access password assigned to your practice. | |
9 |
| How to Handle Non Future Carriers | If a carrier does not allow verification for future dates of service, select if you want to replace the future date with today's date and proceed with verification or if you want to skip the verification. | |
1 |
| Default View | Select the applicable option to indicate the default view for elibibility results. | |
1 |
Copyright and Trademark Notice. Copyright © 2019 CompuGroup Medical, Inc. CGM®, CompuGroup Medical® and the CGM logo are registered trademarks and CGM webPRACTICE™ and CGM webTOOLS™ are trademarks of CompuGroup Medical AG in the United States and/or other countries. Any rights not expressly granted herein are reserved.
