![]()
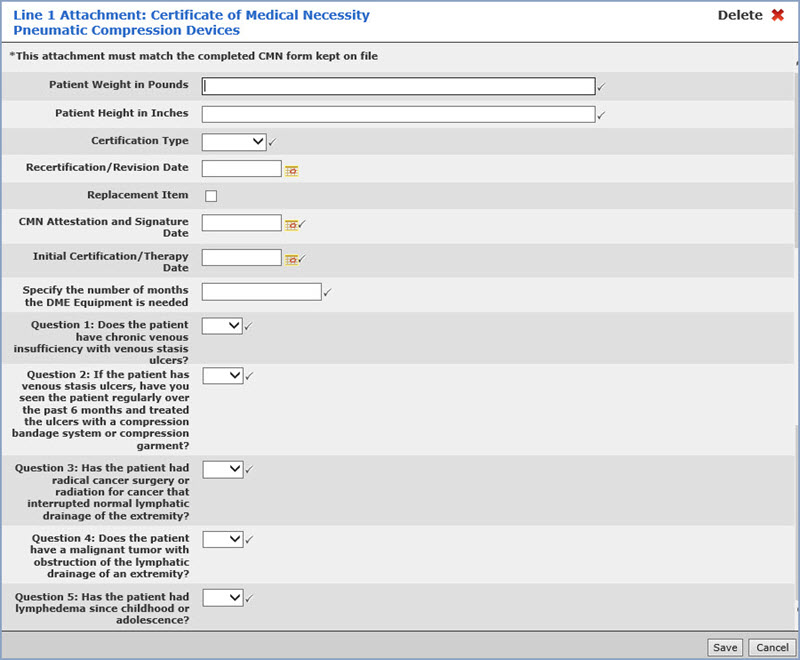
This attachment does not have any specific triggers, but is required for DMERC carriers when this Certificate of Medical Necessity is needed.
| Prompt | Response | Req | Len |
|---|---|---|---|
| Patient Weight in Pounds | Enter the patient's weight in pounds. Populates Loop 2000B, Segment PAT. | 
|
7 |
| Patient Height in Inches | Enter the patient's height in inches. Populates Loop 2400, Segment MEA. | |
4 |
| Certification Type | Select the certification type from the list. Populates Loop 2400, Segment CR3. | |
1 |
| Recertification/Revision Date | Enter the date you want or click the calendar icon to select a date. Populates Loop 2400, Segment DTP*607. | 10 | |
| Replacement Item | If this is a replacement item, select this check box. Populates Loop 2400, Segment CRC. | 10 | |
| CMN Attestation and Signature Date | Enter the date you want or click the calendar icon to select a date. Populates Loop 2400, Segment DTP*461. | |
10 |
| Initial Certification/Therapy Date | Enter the date you want or click the calendar icon to select a date. Populates Loop 2400, Segment DTP*463. | |
10 |
| Specify the number of months the DME Equipment is needed | Enter the number of months. Populates Loop 2400, Segment CR3 | |
50 |
| Question 1: Does the patient have chronic venous insufficiently with venous stasis ulcers? | |
1 |
|
| Question 2: If the patient has venous stasis ulcers, have you seen the patient regularly over the past 6 months and treated the ulcers with a compression bandage system or compression garment? | |
1 | |
| Question 3: Has the patient had radical cancer surgery or radiation for cancer that interrupted normal lymphatic drainage of the extremity? | |
1 | |
| Question 4: Does the patient have a malignant tumor with obstruction of the lymphatic drainage of an extremity? | |
1 | |
| Question 5: Has the patient had lymphedema since childhood or adolescence? | |
1 |
Copyright and Trademark Notice. Copyright © 2019 CompuGroup Medical, Inc. CGM®, CompuGroup Medical® and the CGM logo are registered trademarks and CGM webPRACTICE™ and CGM webTOOLS™ are trademarks of CompuGroup Medical AG in the United States and/or other countries. Any rights not expressly granted herein are reserved.
