![]()
| Prompt | Response | Req | Len |
|---|---|---|---|
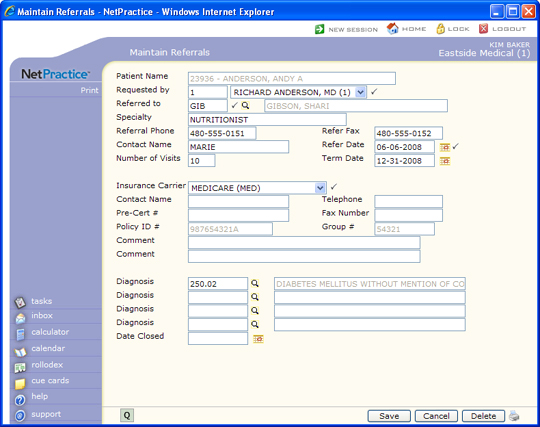
| Requested by | Type the code of the doctor who is making the referral or select from the Requested by list. |  |
5 |
| Referred to | Type the Referral Source code of the provider that the patient is being referred to or click the magnifying glass to search the table. | |
5 |
| Specialty | Type the specialty for the referral source. This field will default with the specialty entered for the referral source code but may be changed as needed. | 30 | |
| Referral Phone | Type the phone number for the referral source. This field will default with the number entered for the referral source code but may be changed as needed. | 20 | |
| Refer Fax | Type the fax number for the referral source. This field will default with the number entered for the referral source code but may be changed as needed. | 20 | |
| Contact Name | Type the name of the contact person at the referral source's office. This field will default with the name entered for the referral source code but may be changed as needed. | 18 | |
| Refer Date | Type the starting date of the referral or click the calendar icon to select a date. | |
10 |
| Number of Visits | Type the number of visits permitted for this referral. | 3 | |
| Term Date | Type the date this referral will expire or click the calendar icon to select a date. This field indicates when the referral expires, regardless of the number of visits used. | 10 | |
| Insurance Carrier | Select the insurance carrier that needs the referral information. | |
5 |
| Contact Name | Type the name of the contact person for the insurance carrier. This field will default with the contact name entered for the insurance carrier code but may be changed as needed. | 18 | |
| Telephone | Type the phone number for the insurance carrier. This field will default with the number entered for the insurance carrier code but may be changed as needed. | 20 | |
| Pre-Cert # | Type the pre-cert number, if applicable. | 18 | |
| Fax Number | Type the fax number for the insurance carrier. This field will default with the number entered for the insurance carrier code but may be changed as needed. | 20 | |
| Policy ID # | This field is informational only and reflects the patient's policy number for the selected insurance carrier. | 15 | |
| Group # | This field is informational only and reflects the patient's group number for the selected insurance carrier. | 10 | |
| Comment | Type any necessary comment text. | 45 | |
| Comment | Type any additional comments about this referral. | 45 | |
| Diagnosis | Type the diagnosis code for this referral or click the magnifying glass to search the table. | 10 | |
| Diagnosis | Type the diagnosis code for this referral or click the magnifying glass to search the table. | 10 | |
| Diagnosis | Type the diagnosis code for this referral or click the magnifying glass to search the table. | 10 | |
| Diagnosis | Type the diagnosis code for this referral or click the magnifying glass to search the table. | 10 | |
| Date Closed | Type the date to indicate that this patient has been seen by the doctor you referred to or click the calendar icon to select a date. This field can also be completed through the Close Outstanding Referrals function. | 10 |
Copyright and Trademark Notice. Copyright © 2019 CompuGroup Medical, Inc. CGM®, CompuGroup Medical® and the CGM logo are registered trademarks and CGM webPRACTICE™ and CGM webTOOLS™ are trademarks of CompuGroup Medical AG in the United States and/or other countries. Any rights not expressly granted herein are reserved.
