![]()
The entry of any one of the following HCPCS codes: A0425, A0426, A0427, A0428, A0429, A0430, A0431, A0432, A0433, A0434, A0435, A0436, A0888 will trigger the Ambulance Attachment.
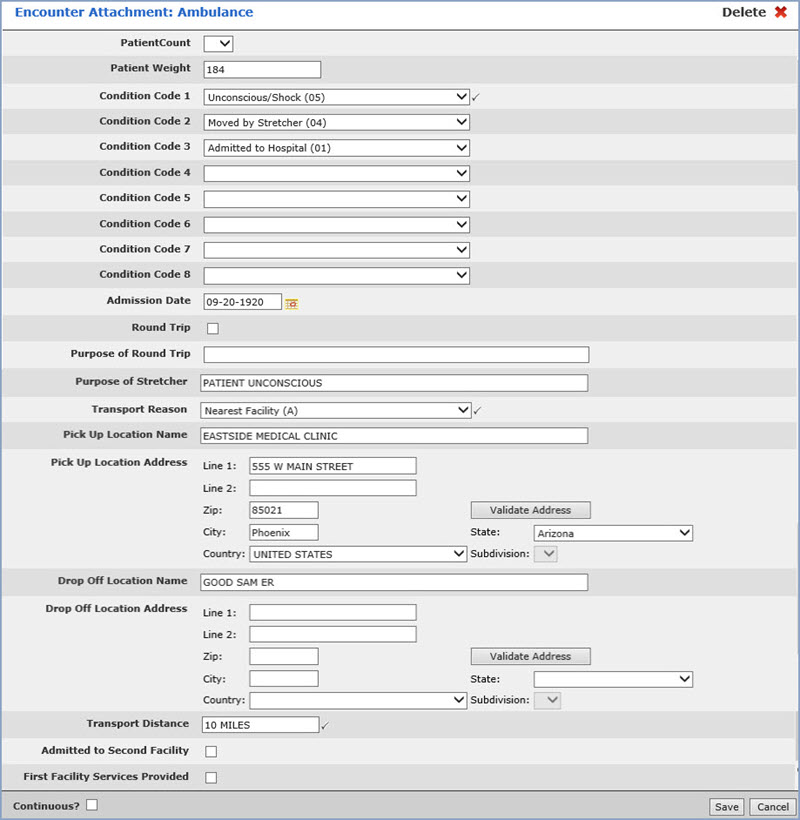
| Prompt | Response | Req | Len |
|---|---|---|---|
| Patient Count | Select the count you want from the list. | 1 |
|
| Patient Weight | Enter the weight of the patient. | 50 |
|
| Condition Code 1 | Select the condition code you want from the list. | 
|
1 |
| Condition Codes 2 through 8 | Select the condition code you want from the list. | 1 | |
| Admission Date | Enter the date you want or click the calendar icon to select a date. | 10 |
|
| Round Trip | If the service was round trip, select this check box. | 1 | |
| Purpose of Round Trip | If you selected the Round Trip check box above, enter the purpose of the round trip. | 80 |
|
| Purpose of Stretcher | Enter the purpose of the stretcher. | 50 | |
| Transport Reason | Select the transport reason you want from the list. | |
1 |
| Pick up Location Name | Enter the name of the pick up location. | 50 | |
| Pick up Location Address - Line 1 | Enter the address for the pick up location. | 50 | |
| Line 2 | Enter any additional address information. | 50 | |
| Zip | Enter the five digit zip code | 50 | |
| City | The city automatically populates based on the Zip Code entered, or you can type the name of the city. | 50 | |
| State | The state automatically populates based
on the Zip Code entered, or you can type the state code or select
from the drop-down list. Click Validate Address to convert the address entered into the standard United States Postal Service format. The Address Line One will be converted; the information in Address Line Two (if standard) moves up to the end of Address Line One; the Zip Code is converted to Zip+4 and the City and State are converted based on the Zip Code. If a standard match cannot be found, messages display to explain. If you disagree with the converted address, you can change it back and save it without the validation changes. These changes will prevent claims from being rejected or added to the Exception report due to an invalid address or state code. |
1 | |
| Country | Enter the country code or select from the Country list. | 1 |
|
| Subdivision | If you selected a country other than the US, select a subdivision from the list. | 1 |
|
| Drop Off Location Name | Enter the name of the drop off location. | 50 |
|
| Drop Off Location Address - Line 1 | Enter the address for the drop off location. | 50 | |
| Line 2 | Enter any additional address information. | 50 | |
| Zip | Enter the five digit zip code | 50 | |
| City | The city automatically populates based on the Zip Code entered, or you can type the name of the city. | 50 | |
| State | The state automatically populates based
on the Zip Code entered, or you can type the state code or select
from the drop-down list. Click Validate Address to convert the address entered into the standard United States Postal Service format. The Address Line One will be converted; the information in Address Line Two (if standard) moves up to the end of Address Line One; the Zip Code is converted to Zip+4 and the City and State are converted based on the Zip Code. If a standard match cannot be found, messages display to explain. If you disagree with the converted address, you can change it back and save it without the validation changes. These changes will prevent claims from being rejected or added to the Exception report due to an invalid address or state code. |
1 | |
| Country | Enter the country code or select from the Country list. | 1 | |
| Subdivision | If you selected a country other than the US, select a subdivision from the list. | 1 | |
| Transport Distance | Enter the distance the patient was transported. | |
50 |
| Admitted to Second Facility | If the patient was admitted to a second facility, select this check box. | 1 |
|
| First Facility Services Provided | If services were provided at the first facility, select this check box. | 1 |
Copyright and Trademark Notice. Copyright © 2019 CompuGroup Medical, Inc. CGM®, CompuGroup Medical® and the CGM logo are registered trademarks and CGM webPRACTICE™ and CGM webTOOLS™ are trademarks of CompuGroup Medical AG in the United States and/or other countries. Any rights not expressly granted herein are reserved.
