![]()
This attachment does not have any specific triggers, but is required for DMERC carriers when this Certificate of Medical Necessity is needed.
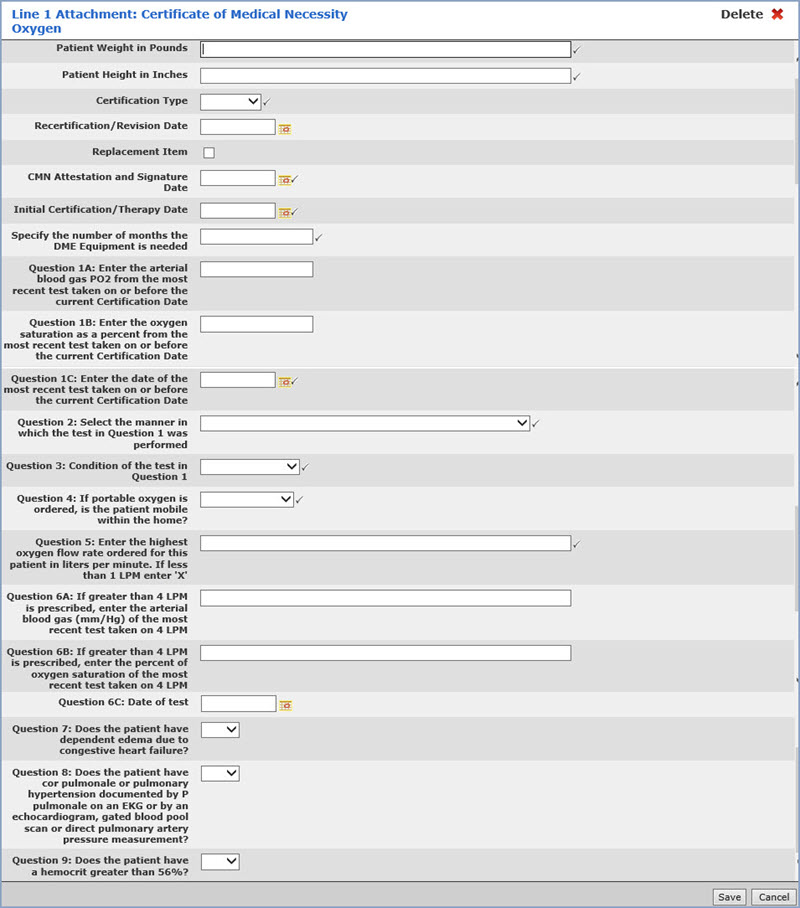
Data Field Information
| Prompt | Response | Req | Len |
|---|---|---|---|
| Patient Weight in Pounds | Enter the patient's weight in pounds. Populates Loop 2000B, Segment PAT. | 
|
7 |
| Patient Height in Inches | Enter the patient's height in inches. Populates Loop 2400, Segment MEA. | |
4 |
| Certification Type | Select the certification type from the list. Populates Loop 2400, Segment CR3. | |
1 |
| Recertification/Revision Date | Enter the date you want or click the calendar icon to select a date. Populates Loop 2400, Segment DTP*607. | 10 | |
| Replacement Item | If this is a replacement item, select this check box. Populates Loop 2400, Segment CRC. | 10 | |
| CMN Attestation and Signature Date | Enter the date you want or click the calendar icon to select a date. Populates Loop 2400, Segment DTP*461. | |
10 |
| Initial Certification/Therapy Date | Enter the date you want or click the calendar icon to select a date. Populates Loop 2400, Segment DTP*463. | |
10 |
| Specify the number of months the DME Equipment is needed | Enter the number of months. Populates Loop 2400, Segment CR3. | |
50 |
| Question 1A: Enter the arterial blood gas PO2 from the most recent test taken on or before the current Certification Date | If the value typed for Question 1A is 55.5-59.4, then Questions 7, 8 and 9 are required. | |
50 |
| Question 1B: Enter the oxygen saturation as a percent from the most recent test taken on or before the current Certification Date | If the value typed for Question 1B is 88.5-89.4, then Questions 7, 8, and 9 are required. | |
50 |
| Question 1C: Enter the date of the most recent test taken on or before the current Certification Date | Enter the date you want or click the calendar icon to select a date. | |
10 |
| Question 2: Select the manner in which the test in Question 1 was performed | Select the applicable manner from the list. | |
1 |
| Question 3: Condition of the test in Question 1 | Select the condition of the test from the list. | |
1 |
| Question 4: If portable oxygen is ordered the patient mobile within the home | Select the applicable option from the list. | |
1 |
| Question 5: Enter the highest oxygen flow rate ordered for this patient in liters per minute. If less than 1 LPM enter 'X' | Enter the highest oxygen flow rate. If the value typed for Question 5 is greater than 4, Question 6A or 6B must be filled in. | |
50 |
| Question 6A: If greater than 4 LPM is prescribed, enter the arterial blood gas (mm/Hg) of the most recent test taken on 4 LPM | If there is a response in Question 6A or 6B, Question 6C (date) must also be filled in. | 50 |
|
| Question 6B: If greater than 4 LPM is prescribed, enter the percent of oxygen saturation of the most recent test taken on 4 LPM | If there is a response in Question 6A or 6B, Question 6C (date) must also be filled in. | 50 |
|
| Question 6C: Date of test | Enter the date you want or click the calendar icon to select a date. | 10 |
|
| Question 7: Does the patient have dependent edema due to congestive heart failure | Select the applicable option from the list. | 1 |
|
| Question 8: Does the patient have cor pulmonale or pulmonary hypertension documented by P pulmonale on an EKG or by an echocardiogram, gated blood pool scan or direct pulmonary artery pressure measurement? | Select the applicable option from the list. | 1 |
|
| Question 9: Does the patient have a hemocrit greater than 56%? | Select the applicable option from the list. | 1 |
Copyright and Trademark Notice. Copyright © 2019 CompuGroup Medical, Inc. CGM®, CompuGroup Medical® and the CGM logo are registered trademarks and CGM webPRACTICE™ and CGM webTOOLS™ are trademarks of CompuGroup Medical AG in the United States and/or other countries. Any rights not expressly granted herein are reserved.
