![]()
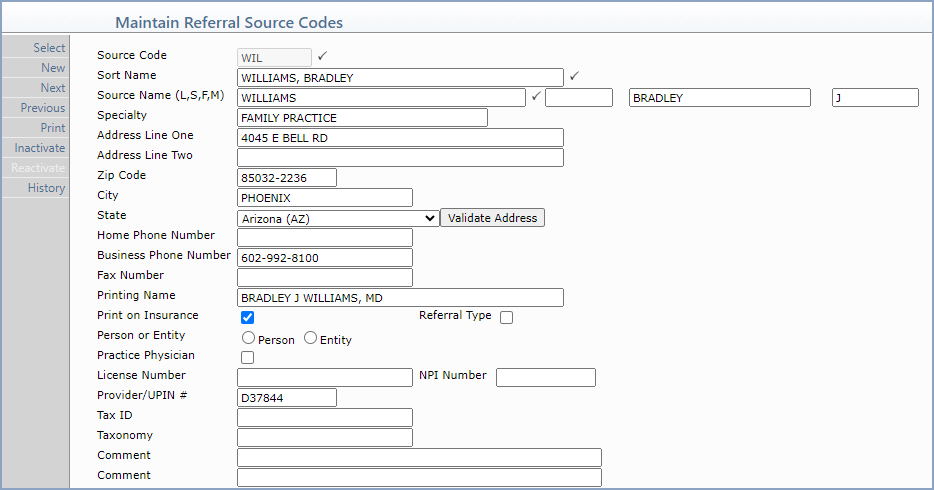
| Prompt | Response | Req | Len |
|---|---|---|---|
| Source Code | Type the code you want or click the magnifying glass to search the table. This code cannot begin with a zero. | 6 | |
| Sort Name | Type the name to be used when sorting referral source codes alphabetically. |  |
40 |
| Last Name | Type the last name of the referral source. | |
60 |
| Suffix | Enter the Source's Suffix. | 10 | |
| First Name | Type the first name of the referral source. | 35 | |
| Middle Name | Type the middle name of the referral source. | 25 | |
| Specialty | Type the specialty for this referral source. | 30 | |
| Address Line One | Type the address for the referral source. | 40 | |
| Address Line Two | Type any additional address information for the referral source. | 40 | |
| Zip Code | Type the zip code. | 10 | |
| City | Type the city and state. It should be entered in the exact format shown. For example, Phoenix, AZ. Type the city name - then a comma - then one space - and the two letter state code. | 20 | |
| State | Type the State. | 3 | |
| Home Phone Number | Type the home phone number for this referral source. | 20 | |
| Business Phone Number | Type the business phone number for this referral source. | 20 | |
| Fax Number | Type the fax number for this referral source. | 20 | |
| Printing Name | Type the name in the format you want to print on any reports and insurance claim forms. | 40 | |
| Print on Insurance | If you want this referral source to print on insurance forms, select this check box. | |
1 |
| Referral Type | If you want to designate this referral source code as a referral type, select this check box. You can then specify a referral type on the Patient Name and Address Information screen in Change Patient Data. | 1 | |
| Person or Entity | Select the option to indicate if this is an actual doctor or if it represents a group or business. This is used for electronic claims | 1 | |
| Practice Physician | If this referral source is a provider in your practice, select this check box so you can differentiate the providers in your practice from outside referring providers. | 1 | |
| License Number | Type the license number issued by the state, if applicable. | 20 | |
| NPI Number | Type the referral source's NPI number. | 10 | |
| Provider/UPIN # | Type the referral source's UPIN number. | 10 | |
| Tax ID | Type the referral source's Tax ID number. | 20 | |
| Taxonomy | Type the referral source's Taxonomy number. | 20 | |
| Comment | Type any necessary comment text. | 45 | |
| Comment | Type any necessary comment text. | 45 |
Copyright and Trademark Notice. Copyright © 2019 CompuGroup Medical, Inc. CGM®, CompuGroup Medical® and the CGM logo are registered trademarks and CGM webPRACTICE™ and CGM webTOOLS™ are trademarks of CompuGroup Medical AG in the United States and/or other countries. Any rights not expressly granted herein are reserved.
