![]()
| Prompt | Response | Req | Len |
|---|---|---|---|
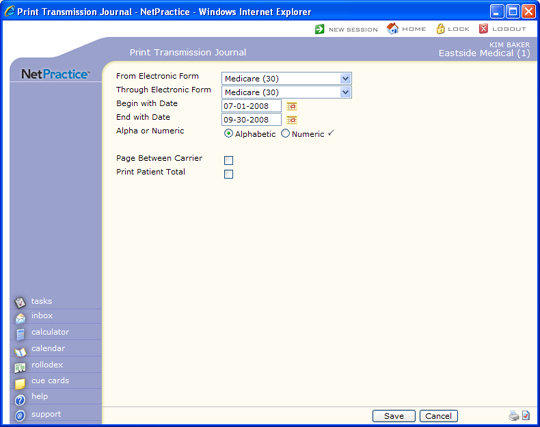
| From Electronic Form | Select the electronic form number you want to start with or leave the field blank to begin with the first code. | 2 | |
| Through Electronic Form | Select the electronic form number you want to end with or leave the field blank to end with the last code. | 2 | |
| Begin with Date | Type the date you want to begin with or click the calendar icon to select a date. This date refers to the date the insurance claim file was created.This date refers to the date the insurance claim file was created. | 10 | |
| End with Date | Type the date you want to end with or click the calendar icon to select a date. This date refers to the date the insurance claim file was created. | 10 | |
| Alpha or Numeric | Select the option to print the patients in alphabetical order by last name or in numeric order by account number. |  |
1 |
| Page Between Carrier | If you want each carrier to begin printing on a new page, select this check box. | 1 | |
| Print Patient Total | If you want to print a total claim dollar amount for each patient, select this check box. | 1 |
Copyright and Trademark Notice. Copyright © 2019 CompuGroup Medical, Inc. CGM®, CompuGroup Medical® and the CGM logo are registered trademarks and CGM webPRACTICE™ and CGM webTOOLS™ are trademarks of CompuGroup Medical AG in the United States and/or other countries. Any rights not expressly granted herein are reserved.
