![]()
| Prompt | Response | Req | Len |
|---|---|---|---|
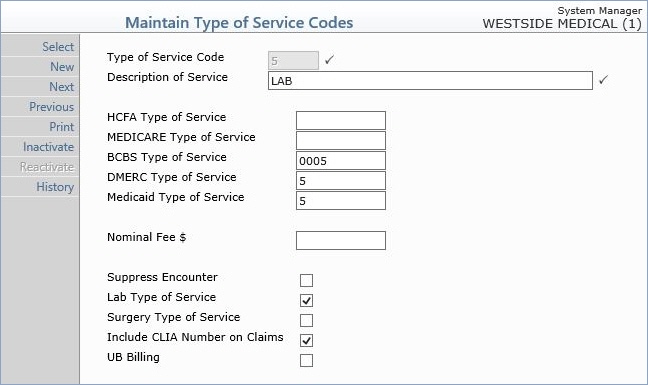
| Type of Service Code | Type the code you want or click the magnifying glass to search the table. This code cannot begin with a zero. | 3 | |
| Description of Service | Type a description of the type of service code. This description defines the type of service for this code. For example, if the code is set to '1', a valid description could be 'Medical Care'. |  |
45 |
| HCFA Type of Service | Type the equivalent type of service code you want to use on insurance claims for this insurance carrier. For more information see the Equivalent Code help section under Introduction, System Processes. | 10 | |
| MEDICARE Type of Service | Type the equivalent type of service code you want to use on insurance claims for this insurance carrier. For more information see the Equivalent Code help section under Introduction, System Processes. | 10 | |
| BCBS Type of Service | Type the equivalent type of service code you want to use on insurance claims for this insurance carrier. For more information see the Equivalent Code help section under Introduction, System Processes. | 10 | |
| DMERC Type of Service | Type the equivalent type of service code you want to use on insurance claims for this insurance carrier. For more information see the Equivalent Code help section under Introduction, System Processes. | 10 | |
| Medicaid Type of Service | Type the equivalent type of service code you want to use on insurance claims for this insurance carrier. For more information see the Equivalent Code help section under Introduction, System Processes. | 10 | |
| Nominal Fee $ | Community Health Centers only - If you charge a flat fee for this Type of Service, type the dollar amount. | 10 | |
| Suppress Encounter | Community Health Centers only - If procedures posted containing this Type of Service code are not considered encounters, select this check box. | 1 | |
| Medicare 100% Reimbursement | If Medicare reimburses this type of service at 100% of the allowable amount (versus the standard 80% of the allowable amount), select this check box. This ensures that Medicare payments for this type of service will be handled correctly in the Payment Entry Function and in the Electronic Remittance Advice (ERA) function. | 1 | |
| Surgery Type of Service | If this is a surgery type of service, select this check box. | 1 | |
| Include CLIA Number on Claims | If you want the CLIA number to go on claims for this type of service, select this check box. | 1 | |
| UB Billing | Rural Health Centers and FQHC's only: If you want to send UB claims for this type of service, select this check box. | 1 |
Copyright and Trademark Notice. Copyright © 2019 CompuGroup Medical, Inc. CGM®, CompuGroup Medical® and the CGM logo are registered trademarks and CGM webPRACTICE™ and CGM webTOOLS™ are trademarks of CompuGroup Medical AG in the United States and/or other countries. Any rights not expressly granted herein are reserved.
