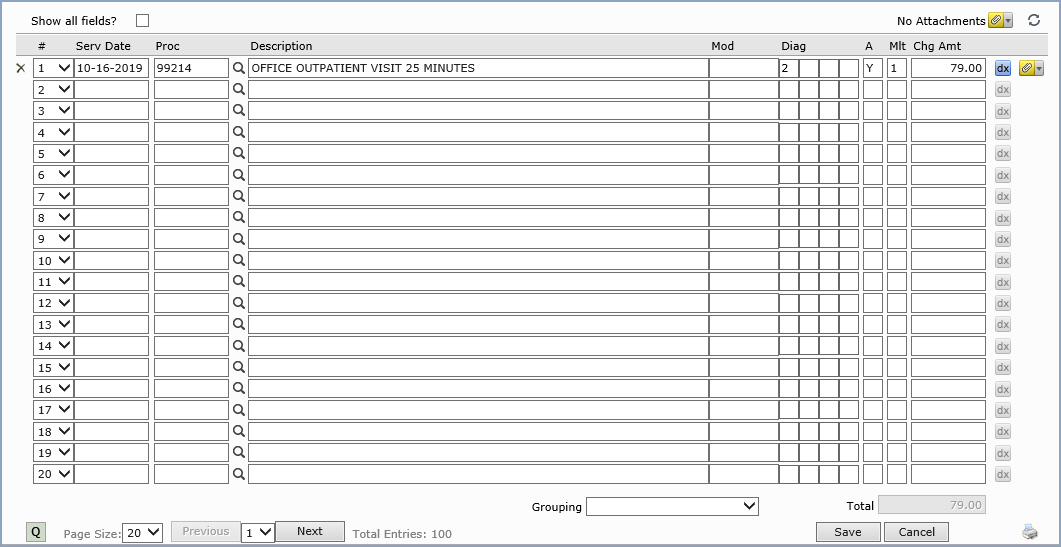
Procedure Entry Screen-Bottom Section
After completing the top section, when you press tab, your pointer will
stop at the Service Date (Serv Date)
field which reflects the date the procedure was actually performed. This
is the date that will be printed on statements and insurance forms. Remember
that it is the Accounting Date that will be used for aging the procedures
and accumulating the statistical information. The default response displayed
for the service date for the first procedure will be the Accounting Date
that was entered. Any subsequent procedures will default to the service
date entered for the previous procedure. You may enter up to 400 procedures
per encounter.
The next field is for the Procedure or CPT code. Your response to
this field must be any valid procedure code from the Procedure Code Table
or you may click the magnifying glass icon to search for a code or add
a new procedure code to the table. When you press tab to accept the procedure
code entered, where the pointer stops next, depends on how you have your
tab stops set up in the Procedure
Entry Integration function. If you don't have any tab stops set up,
the remaining fields will automatically be filled in using: no modifier,
the diagnosis codes entered in the top section, a multiplier of 1, and
the charge amount based on the values stored for the procedure code in
the procedure code table. If you do have tab stops set up, your pointer
will stop at the selected field and allow you to modify the entry.
Procedure Grouping - On the bottom portion of the screen you will
notice a drop down box labeled Grouping. This list box contains all the
Procedure
Grouping codes created for your practice. Click the arrow on the list
box to display the available grouping codes.
If you select a grouping, all procedures contained in
that grouping will automatically be displayed on your screen. This is
extremely helpful when codes have to be bundled or for combinations of
codes that are often billed out together.
If the Check for Duplicate Transactions field
is selected in the Procedure
Entry Integration function, CGM webPRACTICE will check to see if the
procedure you just entered has already been posted to the patient's account
within the last 90 days. If it has, you will receive a warning message.
The Description field will display the complete description of the
procedure selected as defined in the Procedure Code Table. You may type
your own description for more detail. Forty characters are allowed for
your description. Anything typed into the description field will override
the Procedure Code Table description. This description will print on patient
statements and will be displayed when reviewing the patient's transaction
history. When you advance to the next field, the brief description from
the table will automatically replace the full description (if the table
description was accepted). If you typed in your own description, the characters
entered will be shortened to twenty. Your entire entry will be maintained
within CGM webPRACTICE, but needs to be shortened at this time to allow
room for the additional responses.
There are certain special procedure codes that require you to type data
in the description field. After you type the procedure code, the pointer
will automatically focus on the description field and require you to type
the applicable data. Some of the codes included are; AUTH-authorization
numbers, NOTE-notes, TIME-anesthesia time, PS-purchased services. For
detailed instructions, see the Special
Procedure Codes section.
The Modifier is an optional field that you can use to enter any
procedure code modifiers necessary for insurance submission. You may type
up to three, two digit modifier codes. The codes should not be separated
by dashes or commas when typed. For example, to type the three modifiers
'22', '51', and '80' they should be typed as '225180'). To force electronic
claims to the paper file, type 'PP' as the modifier. Those claims will
be listed on the Exception
Report with the reason of ' Paper Submission Due to Modifiers'. You
can type the 'PP' by itself or in addition to other modifiers.
In
the four Diagnosis Pointer fields on each line item, you can make
reference to the specific diagnosis codes (entered in the top portion
of the screen) that apply to this procedure. Only one diagnosis pointer
(1-12) should be entered per field. The first pointer entered should reference
the primary diagnosis for the procedure. You can change the order of reference
for each procedure, if necessary, which could affect your reimbursement
from the insurance carrier.
You can crosscheck
procedure codes against diagnosis codes using the CPT®/DX
Cross Linking Table. If you link a diagnosis code
to a procedure code in the CPT®/DX
Cross Linking Table and
in Procedure
Entry you enter a procedure code without having entered one of its
linked diagnosis codes, a message appears. This is a warning only and
you can continue entering the procedure. When this message displays, the
dx
icon on the line item is activated.
Click the dx
icon to view a list of all the valid diagnosis codes that are linked to
the procedure code. You can then select a code from the list by clicking
it and then clicking Save
or by double-clicking the code. The selected diagnosis code will be inserted
in the top portion of the screen and the appropriate diagnosis pointer
will be inserted for the procedure line item.
The defaulted
diagnosis pointers represent all of the diagnosis codes entered in the
top portion of the screen, in the same order (up to four), unless the
procedure code is linked to one of the diagnosis codes in the CPT®/DX
Cross Linking Table or
you selected a linked diagnosis code, or if the procedure code has a Default
Diagnosis entered in the Procedure
Code Table. If you enter a Default
Diagnosis code on a procedure in the Procedure
Code Table, that code will default when that procedure code is
entered. At least one diagnosis pointer is required on each procedure
line item to Save
the encounter. If no pointers exist, a message will display informing
you which procedure line item requires a pointer.
Hierarchy
for Diagnosis Pointer field population:
The following
are listed in the order of priority and as soon as a match is found the
pointers will be inserted and no further match checking will be performed.
- If there is a diagnosis
code(s) in the CPT®/DX Linking Table that exists for the procedure code
entered and the diagnosis code(s) has been entered in the top portion
of the screen, the diagnosis pointer(s) for the diagnosis code(s)
will be inserted.
- If
the procedure code has a Default
Diagnosis entered in the Procedure
Code Table,
the
diagnosis code will be inserted in the top portion of the screen and
the appropriate diagnosis pointer will be inserted for the procedure
line item.
If
diagnosis codes have been entered in the top portion of the screen,
up to four diagnosis pointers will be inserted for the procedure line
item, in the same order they were entered in the top portion of the
screen.
The A column contains the accept assignment indicator. A default
response exists, but you can change it. The Y (Yes) or N
(No) response that defaults in this field is based on a number of fields
throughout CGM webPRACTICE. For more information, see Accept
Assignment Protocol.
The multiplier field is used to indicate the number of times the
procedure was performed. The default response displayed is a '1'. If any
other number is entered at this prompt the charge amount for the procedure
will automatically be multiplied by the number entered. For correct reimbursement
from the insurance, it is very important to enter the correct multiplier
or number of units here rather than inflating the price.
The last item filled in is the charge amount. This field indicates
the amount to be charged for the procedure. You may either accept the
default charge amount displayed, or you may override the default displayed
with any other amount. There are several different places the default
amount displayed could be coming from. Examples of each are explained
below:
- In the simplest form, each procedure code has a Normal Price defined
in the Procedure
Code Table. If no other circumstances affect the Normal Price
in the Procedure Code Table, that is the amount that will be defaulted
in the Charge field.
- The Procedure Code Table also allows up to five other "normal"
rates to be entered. These other rates (referred to as Rate Schedules
in the Procedure Code Table) must be used if more than one doctor
exists in the practice but each doctor does not charge the same amount
for each procedure. If that is the case, each doctor would be assigned
to a specific Rate Schedule. It is through the Rate Schedule in the
Procedure Code Table that each doctor's normal price for each procedure
is defined. If the performing doctor is assigned to a Rate Schedule,
and no other circumstances affect the normal price for that doctor,
that is the amount that will be shown in the Charge field. If no amount
exists in that doctor's Rate Schedule for the procedure performed,
the amount that would be defaulted is the Normal Price for that procedure.
- For various reasons the need may exist to bill certain groups of
patients with amounts other than the normal fees (i.e., Medicare patients,
industrial patients, etc.). CGM webPRACTICE allows you to maintain
separate sets of fees for billing these certain groups of patients.
These fees are referred to as the alternate fees and they are maintained
in the Fee
Schedule Tables. If the patient currently being billed is assigned
to one of these Fee schedules, the alternate fee amount contained
in that Fee Schedule for that procedure will default in the Charge
field. If no alternate fee existed in the Fee Schedule for that procedure,
the amount that would be defaulted in the Charge field is the amount
contained in the Procedure Code Table. In addition to having a normal
alternate fee in the Fee Schedules you may also have alternate fees
for the doctor's different Rate Schedules (if they also differ). If
a patient is assigned to a Fee Schedule and the performing doctor
is assigned to a Rate Schedule, the alternate fee contained in the
Fee Schedule for that doctor's Rate Schedule is the amount that would
be defaulted. If the doctor does not have an alternate fee defined
in the Fee Schedule for the procedure performed, the amount that will
be defaulted during procedure entry is the amount defined as being
the normal alternate fee for that procedure. If a normal alternate
fee is also not defined the Rate Schedule amount from the Procedure
Code Table will be the default in the Charge field.
If you have your tab stop set at the amount field, once you tab off of
the amount field, the DX button will once again be activated. Pressing
tab once more will bring you back to the next Service Date prompt. You
will continue the process until you have all charges entered for this
patient.
The quickest method to delete all the fields for a procedure is to position
the pointer on the field you want to delete and click. When the procedure
code is highlighted, press the Delete key and then Tab.
Note: if you change the CPT or the multiplier field, the amount will also
change accordingly.
Click Save after you have completed entering all the procedures.
The procedures you just entered are immediately posted to the patient's
transaction history, the statistical records, and the aging records.
