![]()
| Prompt | Response | Req | Len |
|---|---|---|---|
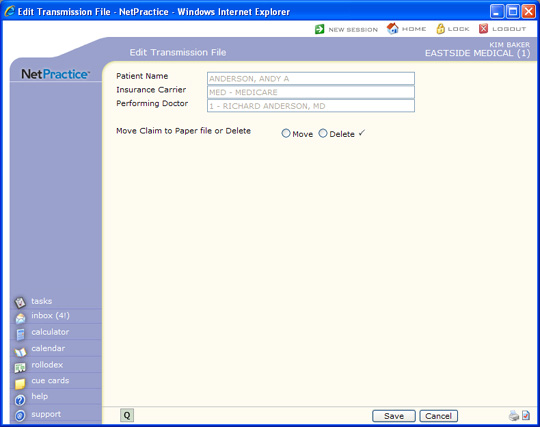
| Insurance Carrier | This field is informational only and reflects the insurance carrier code and name. | 40 | |
| Performing Doctor | This field is informational only and reflects the performing doctor's code and name. | 40 | |
| Move Claim to Paper file or Delete | Select the editing option you want. |  |
1 |
Copyright and Trademark Notice. Copyright © 2019 CompuGroup Medical, Inc. CGM®, CompuGroup Medical® and the CGM logo are registered trademarks and CGM webPRACTICE™ and CGM webTOOLS™ are trademarks of CompuGroup Medical AG in the United States and/or other countries. Any rights not expressly granted herein are reserved.
